
Research Article | DOI: https://doi.org/10.31579/2692-9392/095
Senior Consultant
Department of Emergency Medicine, Singapore General Hospital
Professor, Duke NUS Graduate Medical School
Professor, Yong Loo Lin School of Medicine, National University of Singapore
Professor, Lee Kong Chian Medical School, Nanyang Technological University
Director, Sing Health Duke NUS Institute of Medical Simulation (SIMS)
*Corresponding Author: Fatimah Lateef, Dept of Emergency Medicine, Singapore General Hospital.
Citation: Fatimah Lateef (2022). Evisceration Secondary to Coughing in a Child Undergoing Ventriculoperitoneal Shunt Surgery. J. Archives of Medical Case Reports and Case Study, 5(1); DOI:10.31579/2692-9392/095
Copyright: © 2022 Fatimah Lateef, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 November 2021 | Accepted: 27 December 2021 | Published: 05 January 2022
Keywords: 'kaleidoscopic’ visual aura; migraine; fortification spectrum
This is a case of migraine, presenting with the interesting visual aura of a ‘kaleidoscope’: waves with flickering movements made up of a variety of colors (red, blue, green, yellow), commencing laterally and spreading superiorly in the visual field of the left eye. This description is quite similar to a fortification spectrum, which usually expands and spreads in a C-shape fashion over one side of the visual field.
Several different possible pathophysiological explanation are shared as well as the common differential diagnoses. In the work up of a patient with visual aura migraine, a comprehensive and detailed history is important, together with the appropriate investigations, in order not to miss any serious syndromes, including stroke syndromes and epilepsy.
A 54 year old lady with a history of migraine for many years (where she only has headaches), presented with new onset visual symptom. There was narrowing of the visual field in her left eye, whereby the area affected was the outer and lateral part of the visual field. At the same time, she noticed wave-like, flickering movements comprising of variety of colors (red, blue, green and yellow), commencing laterally and slowly spreading to the superior part of the visual field in her left eye. She described this as an appearance she had seen through a ‘kaleidoscope’. There were no associated scotomas or sudden blindness and she was still able to identify normal images whilst experiencing the attack. She has observed this only in the last 6 months, with the attack coming on about once a month. Each episode would last about 15-20 minutes. The visual symptom started first and is followed by the headache. By the time the headache comes on, the visual symptoms would have subsided. The headache may last anything between 30 minutes to several hours. There was one occasion when she developed vertiginous giddiness after the visual aura symptom. There were no sensory or motor disturbances associated with these attacks. Also, the attack has only happened in her left eye and never in the right eye, thus far. The patient has never been on any regular drugs nor medications. For her migraine, she takes a combination of paracetamol, diclofenac and prochloperazine as needed. The only significant family history is her mum who has a history of migraine, without any visual aura.
At presentation, the examination of the patient was completely normal: stable vital signs, no fever, no localizing cranial nerves or neurological signs. Her blood investigations, full blood count, electrolytes, renal function, thyroid function test, liver function test and calcium-magnesium-phosphate were all normal. Her ESR (erythrocyte sedimentation rate), protein S, protein C, anti-thrombin III factor and antiphospholipid antibody were all normal. The CT scan and Magnetic Resonance Imaging (MRI) of the brain (done after the attack) were also normal. An EEG (electroencephalography) done was also normal.
A final diagnosis of Migraine with Visual Aura was made.
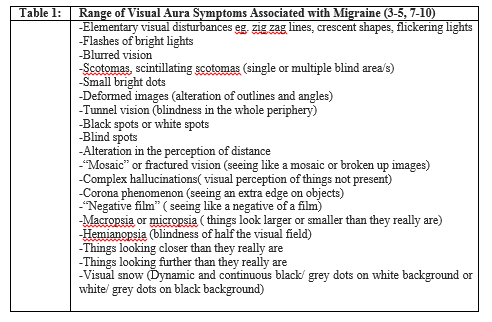
Migraine is a common headache presentation, of varying severity and nature. It is more common in women and can occur either without or with aura, which are usually completely reversible. Migraine triggers are quite common and is reported by some 80% of migraine patients. Change in weather, intake of certain types of food, lack of sleep, certain drug and trauma can be triggers. Aura symptoms may manifest either as sensory, visual or language (or aphasia) disturbances. [1-3] Visual auras are usually the commonest and the most multifaceted. A wide spectrum and range of visual manifestations have been reported in the literature (Table 1). [3-5, 7-10]
Our patient would be classified as having migraine with aura. [1] Such patients can still have a migraine attack without aura as well. The patient’s visual symptoms with flickering, bright and multi-colored waves of lights appear to fit into the description of a ‘fortification spectrum’ that usually expands in a C-shape over one side (lateral aspect) of the visual field, only in her left eye, thus far. The gradual spread that she described is one of the more typical feature of a migraine aura. These visual symptoms are fully reversible. The duration of her aura lasted less than an hour, which is the usual. If the aura lasted more than 60 minutes, it would be classified as a persistent aura without infarction. [3,4, 7-9]
Visual aura usually last between 10-30 minutes. Kaleidoscopic hallucinations are thought to originate in the prestriate area of the brain whilst the zigzag patterns of teichopsia is generated in the striate cortex. This usually is seen in the peripheral vision as wavy images or even dazzling fragments. The brain creates the visual hallucination of ‘fractured’ or bright lights similar to the image when looking through a kaleidoscope. Others have described it as “dancing grains of light”. This is often a short-lived distortion of image and as in our patient, only lasted a few minutes. Kaleidoscopic hallucination as this can affect either one or both eyes, but usually unequally. It commences from the side (lateral aspect of the visual field) and ‘marches’ inwards. The headache may come on with the visual aura or after it has subsided. [3, 10-12]
Differential Diagnoses and Pathophysiology
For a patient presenting with visual aura migraine such as the kaleidoscopic visual aura, for the first time, a work up will be necessary. Transient ischaemic attacks, stroke or a cerebro-vascular event would have to be ruled out. It can also be associated with serious brain injury in a trauma patient. Sometimes this can also be a first presentation for multiple sclerosis (MS). In the approach to the patient, the possibility of retinal migraine (ocular migraine) must be considered. Ocular migraine causes brief attacks of visual symptoms such as flashing, which are usually short-lived and not associated with organic causes. In the rare case of ocular migraine, there may be associated reduced blood flow, which may have some consequence on the retina blood supply. It is thought to be associated with smoking, hypertension, hypoglycaemia or stress. Besides this, ocular migraine can present with scotomas and transient loss of vision. Epilepsy would also have to be ruled out and performing an EEG (electroencephalography) is part of the work up as well. In fact, there is a term, migralepsy, which has been coined and is used to describe a seizure occuring during or within 1 hour of a typical migraine with aura attack. [6, 11, 13-15]
The pathophysiology of the visual auras has been said to be due to one or a combination of the following: [8-10, 16-25]
In the literature, there has also been a case report on kaleidoscopic visual illusions in a patient using stimulant-containing diet pills. Interestingly, this patient’s brother also had the same symptoms when he was abusing stimulant agents, but the symptoms stopped when he stopped using these. [11]
Whereas the brainstem trigeminal nuclei is well known to be involved in the pathophysiology of migraine without aura, there is no conclusive studies or reports to date pertaining to patients with migraine aura. In summary, resting electric and magnetic activities may help to differentiate migraine with and without aura. [10, 21, 27, 28]
In the approach to a patient presenting with migraine with aura, it is important to get a comprehensive history and rule out possible differential diagnoses. Whilst having arrhythmia such as atrial fibrillation (AF) can predispose one to stroke and transient ischemic attacks (TIA), many older patients and those with conditions such as valvular heart disease may have both AF and migraine. Symptoms such as homonymous visual disturbance can happen in both stroke and migraine as well. [6, 18] On the other hand seeing ‘colors and zig zag lines’ are more likely due to migraine aura. Information in the history such as patent foramen ovale, occipital epilepsy and list of drugs patients are taking can be very useful. [6,14, 24, 26]
For the visual aura which is persistently long (>2 hours) it is important to rule out infarction. This is very rare as most visual aura last less than 60 minutes. It is also useful to be aware of the definition of ‘migraine aura status’; ie. experiencing 3 aura within 3 days, although this is also very rare. To rule out differentials such as occipital lobe epilepsy, performing an EEG (electro-encephalography) will help differentiate this from migraine aura. If unsure in any circumstances, it will be better to admit the patient for further investigations. [2,8, 12, 14]
A variety of visual aura manifestations can occur with migraine. It is useful to be aware of this spectrum. Kaleidoscopic visual aura in migraine, as described here, is unique and interesting. To date there are several postulations but not a common consolidated agreement about what causes and where the exact cascade of events brings forth migraine aura, lest to say, specifically with kaleidoscopic visual aura as in this case.
Our patient is receiving further investigations and regular follow up with the Neurologist for her condition.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
